
How might we help families cope with terminal illness?
Using research and physical and digital products to explore healing
- Product: Product and service design for Hum for the ‘Design for End of Life’ course at Parsons School of Design
- Role: Co-screenwriter, film editor, product manager, researcher, strategist
- Software: Adobe Premiere, Google Drive, PowerPoint
- Team: Ankita Roy, Javiera Arenas
Situation
It’s an irony – we often feel like we’re divided and so different from others, when in fact we’re unified in one unchanging fact – we will all face death.
The stigma and complexity of end of life and terminal illness makes this already emotional issue incredibly difficult to deal with. Emotions and loss are some of the hardest moments we can face as individuals, and even when we have support systems like families, few of them have to tools and are equipped to deal with the complexity of such a devastating topic. How can we help families deal with the crisis in family cohesion that can happen after the diagnosis of a terminal illness? How families cope with end of life is an illustration how many of us think about dying. Families live a rescue culture – rescue and all medical treatment, at any cost. The question is, what is the emotional cost of that rescue culture, of crisis, of conflict and of fighting? Social design using the Hum system is one such intervention to create stronger families to address those ruptures to find hope.
Many issues arise among caregivers with a member who has been given a diagnosis of a terminal illness. Some of these issues include:
- A contrast of values: Different personalities, coping mechanisms and goals can lead to conflict between members; a lack of shared responsibility and leadership can lead to caregiver burnout
- Lack of safe space: Nervous energy around caregiving with no means to channel it or no places to go to for certain conversations
- Family conflict or rupture: Fear of uncertainty and the unknown, and difficulty in having serious conversations
- Ritual of intensification: the healthcare system’s rescue culture can lead to a misalignment of goals, expectations and values, and can cause pressure to occur in an already heightened situation
These issues are far more complicated than can be covered in this case study, but they ended up being proof that this project would allow me to work on a deeper level than I’ve ever worked on before.
Research
We used a number of methods to understand the complexity of issues, using secondary research methods, primary/contextual research but also some participatory research. We conducted primary and secondary research for multiple stakeholders and user groups, including interviewing a Memorial Sloan Kettering Cancer Care Hospital patient and family coordinator, Gilda’s Club’s executive director, a hospice nurse and families who are currently or previous dealt with a terminal illness. We also devoured numerous films, literature and journal articles. One highlight for me was the book ‘Speaking of Death: America’s New Sense of Mortality‘, that helped lead me to the value of symbolic meaning.
Secondary research
Research about the current state of end of life care
Much of our desk research involved information about healthcare system and end of life care in general (the ‘as is’ state) and I came up with research questions especially targeted to the domain experts who deliver end of life service care in community, as opposed to palliative care in general. The objectives with the method was to understand the larger systems of healthcare to better understand the gaps in care especially for those families who face end of life challenges for loved ones. This involved looking at care both from researchers who study it as well as the lens of hospitals and other institutions that provide care. The outcome of this method was better clarity in what happens now and what area to focus in on – patients, medical professionals or family members as primary users.
Contextual research
- Interviews with families, end of life community support services
- Site visit to end of life community center
This involved speaking both with family members but also experts who have community care services, including speaking to an incredible staff member at Gilda’s Club and Memorial Sloan Kettering. I devised the questions and the team sat down with both of these people to better understand what the challenges they experienced. We also had team members interview people who had loved ones – family members whose work was invaluable here. The outcome was a renewed focus on creating supports for families; patients need so much help, but silent caregivers can quickly burn out in the life of being a caregiver, and our work was focused on creating supports for the family as a whole.
Participatory research
We held a workshop that both evaluated our prototypes to date and had a larger discussion of what we had found and were thinking of. The outcome of this methods was understanding a lot of the physical requirements that needed to shape an intervention for multiple participants in a family, and what we could create that shaped the branding of our work.
Our research lead to insights that would go towards creating design principles to guide our future work, narrow our scope and solidify our area for prototyping. We also sought to build on the work of William Breitbart at Memorial Sloan Kettering and the concept of ‘meaning centered therapy’ – which tied our focus on meaning to an actual therapeutic practice. My role in the early stages was on understanding attitudes about terminal illness and the search for meaning as a possible focus. All of this would shape the Design Principles, and start to live in the multiple documents we created to share our research findings.
Design principles
Design principles guided our vision and principles for our project:
- Emotion:
- Principle: Accommodate diversity of emotional responses
- Guiding question: How can we create physical and emotional spaces to explore the emotional responses in complex situations?
- New situations:
- Principle: Encourage acceptance of ‘new normals’
- Guiding question: How can we transfer nervous energy to living in the present?
- Acceptance and comfort:
- Principle: Reframe what it means to be comfortable
- Guiding question: How can we allow people to contribute in ways they feel most comfortable?
A lot of this work ultimately lead to exploring in what ways might we cultivate rituals that help families prepare for tough conversations. Then we stumbled on what would be a final version of our How Might We statement: In what ways might we use rituals to encourage the fluidity of roles in order to cultivate shared leadership.[
Wheel of Reason
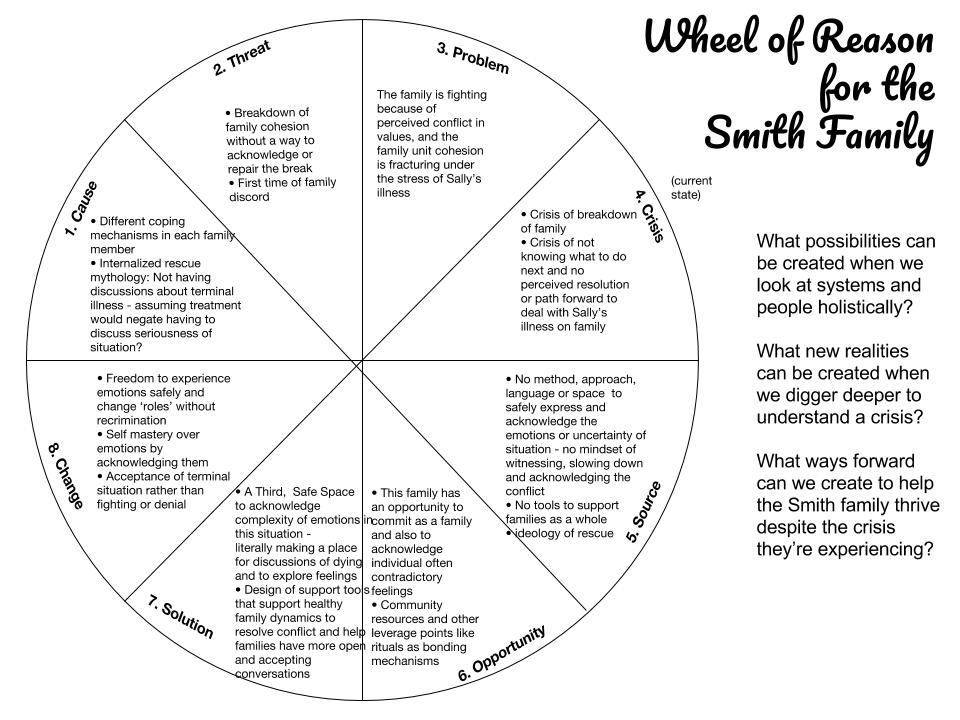
The ‘Wheel of Reason’ became a way for us to understand the situation in greater depth and begin to find a way to approach a solution. This is a great method to ensure we’re thinking holistically about a situation and to drill down to true root causes and challenge our assumptions, especially important in an emotionally charged topic.
Analysis of needs
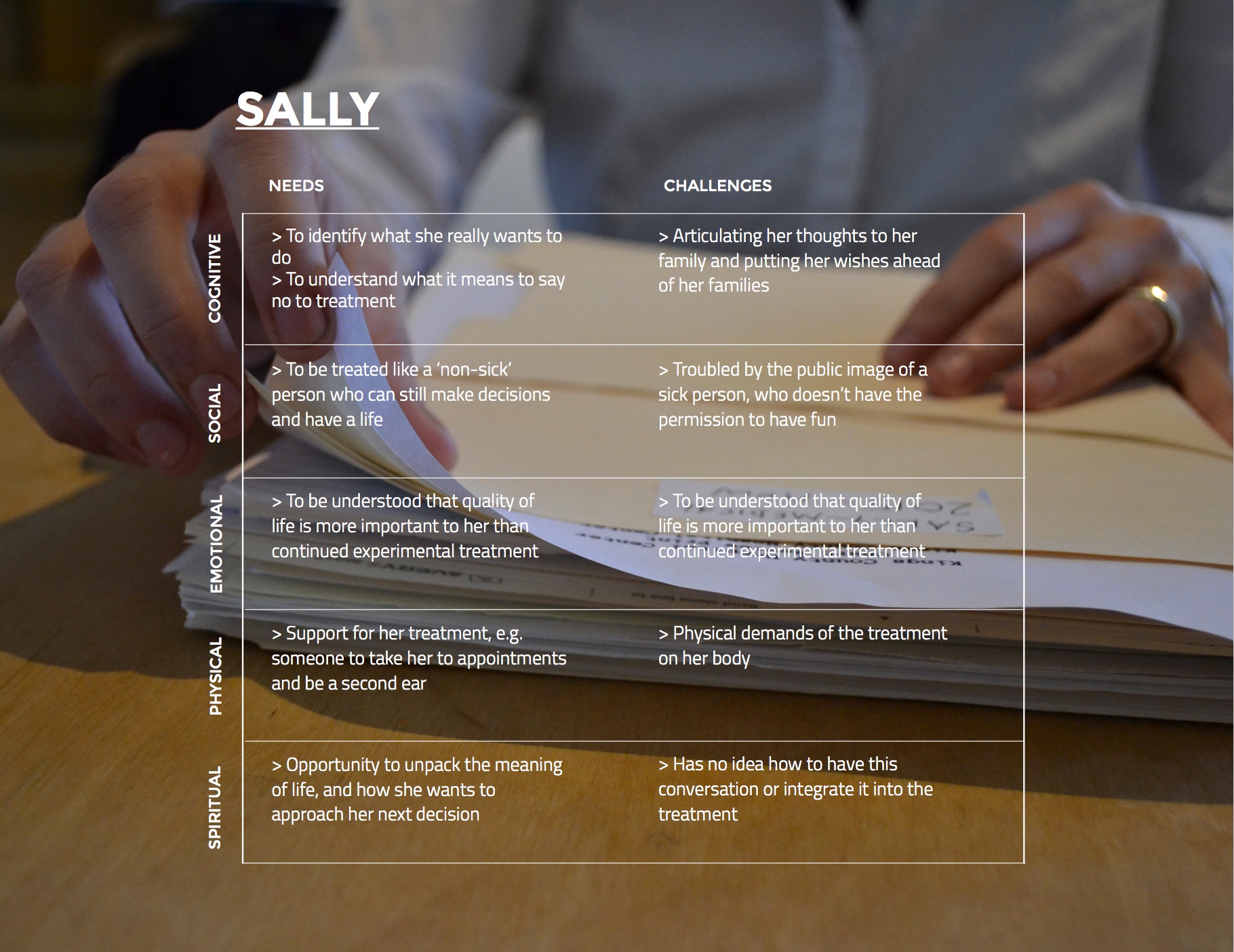
As part of our research we created analysis on the needs and challenges for each character in our script – Sally, the patient and mother, but also the needs and challenges for Mark (her husband) and Kate and Ben, her two children. It was important for us not only to show the perspectives of multiple stakeholders, but to be able to tie our analysis into our eventual design intervention by understanding how each of these different users would ‘use’ our design intervention, something we’d be hinting at in our second film, the ‘ideal’ or ‘future’ state. Photo and its analysis courtesy Ankita Roy.
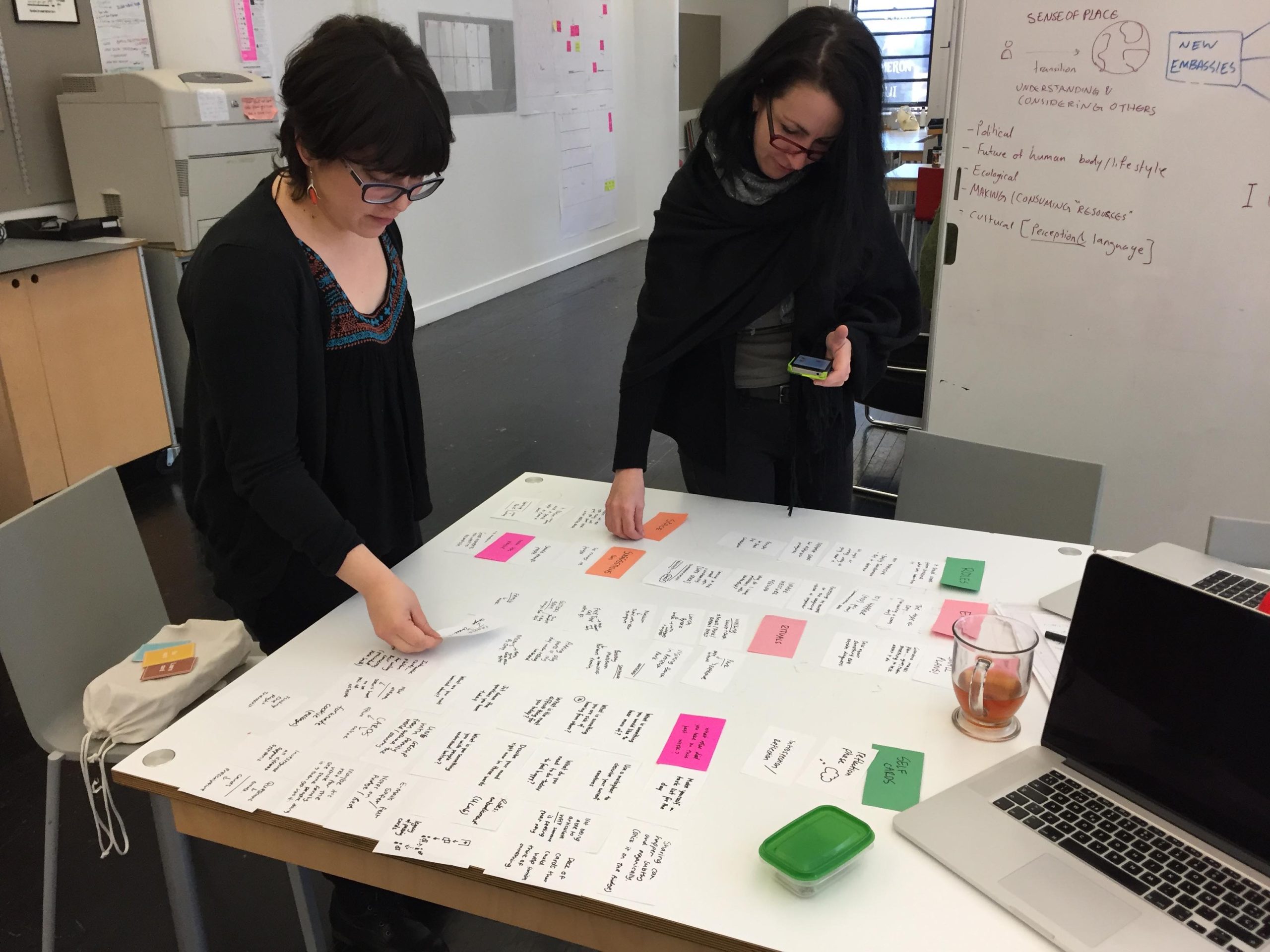
Presenting our findings about the people in our system

This is myself, Ankita and Javi on the left presenting our research on our mythical family – mom ‘Sally’, dad ‘Mark’, son ‘Ben’ and daughter ‘Kate’ . I experimented with how to share our findings, and created table settings for 4 ‘personas’ in the cafe space by our studio, and created objects and clothing to bring our characters to life. The objects and ways we dress reveal our personalities, and creating this was a highlight of the project. Rather than creating static personas, seeing Sally’s pearls and large medical file folder tells you a bit more of the realistic emotional details of a person’s life. (Photo courtesy Winnie Chang)
Our first prototype
I came up with the idea of having a ritual – something involving a card deck with activities for caregivers and a ‘board’ as well as a space as part of the service.
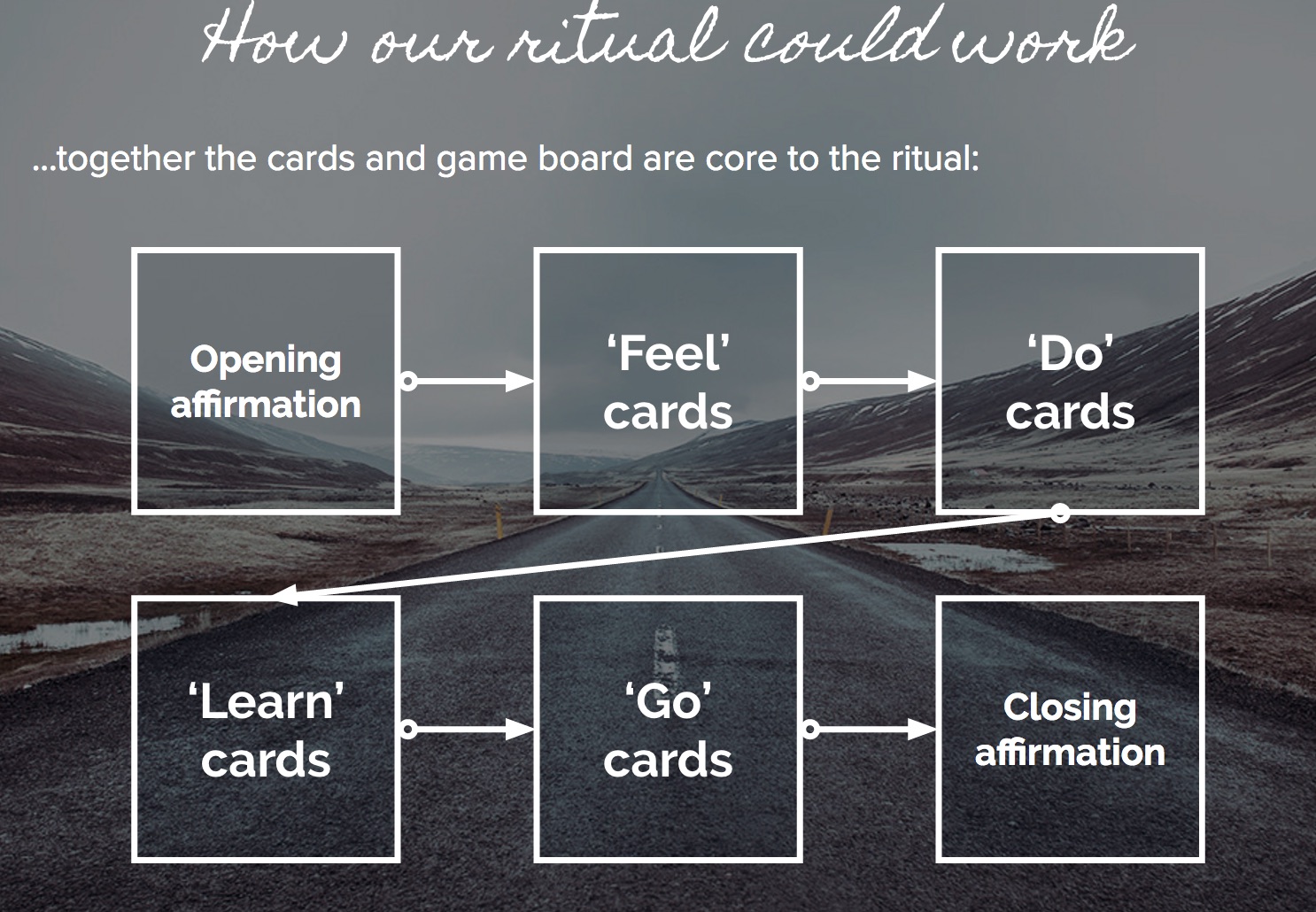
In our midterm presentation we created an early version of Hum that was very ‘ritualized’ and formal:
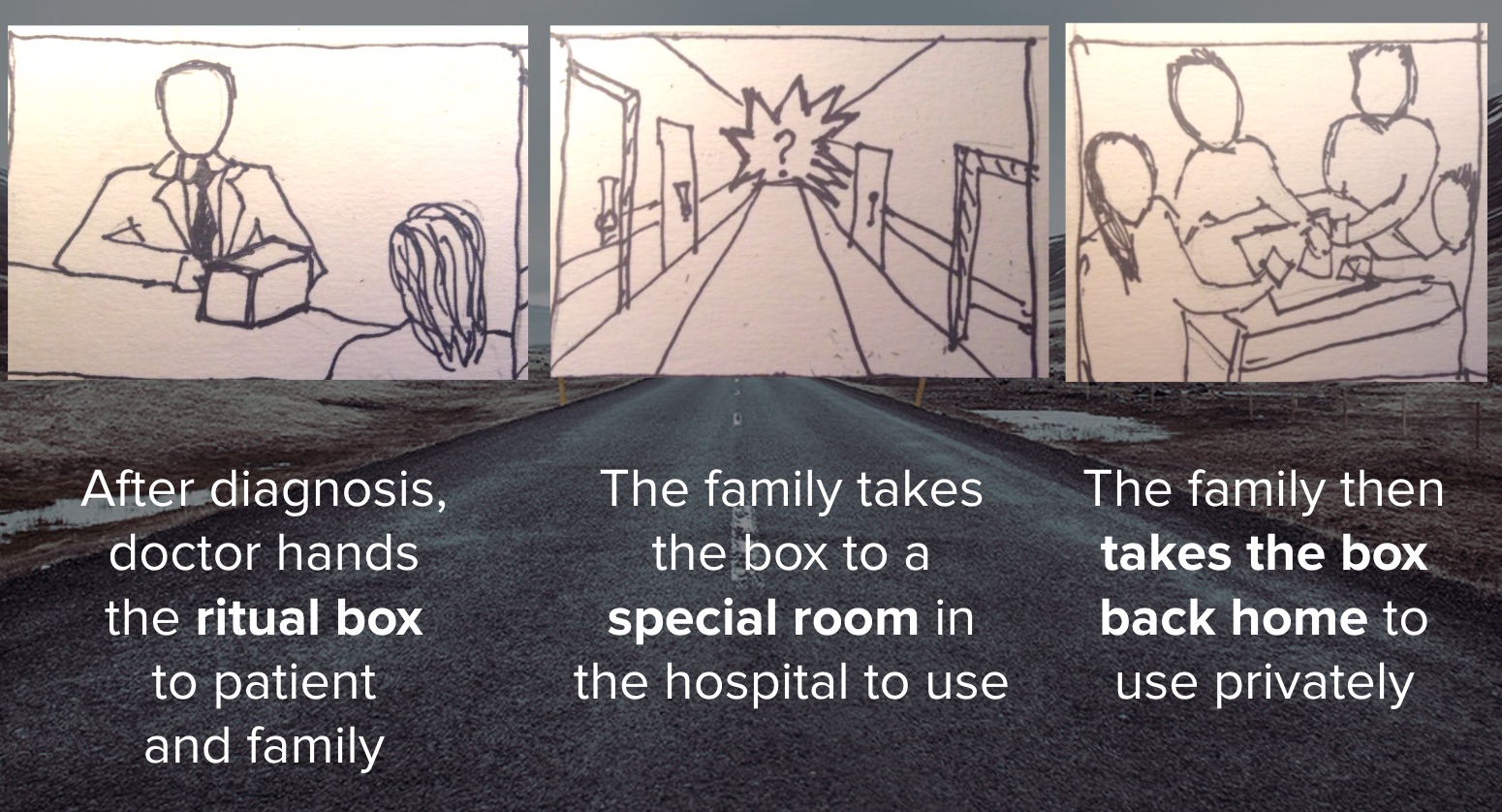
This is a high level view of how the ritual would work as we sought to explore the role of space – in this case, within a medical facility.
The early cards that go in the box were something I created quickly for a workshop. I was exploring the concept of action cards – feel, learn, do, go, with accompanying tasks in each category. Although visually calming, the branding was a little too ‘New Agey’ in this version.
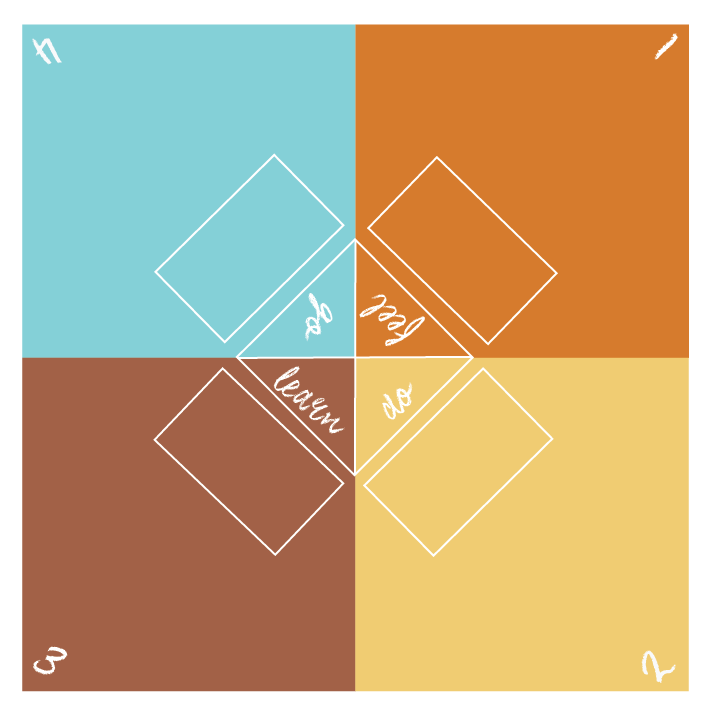
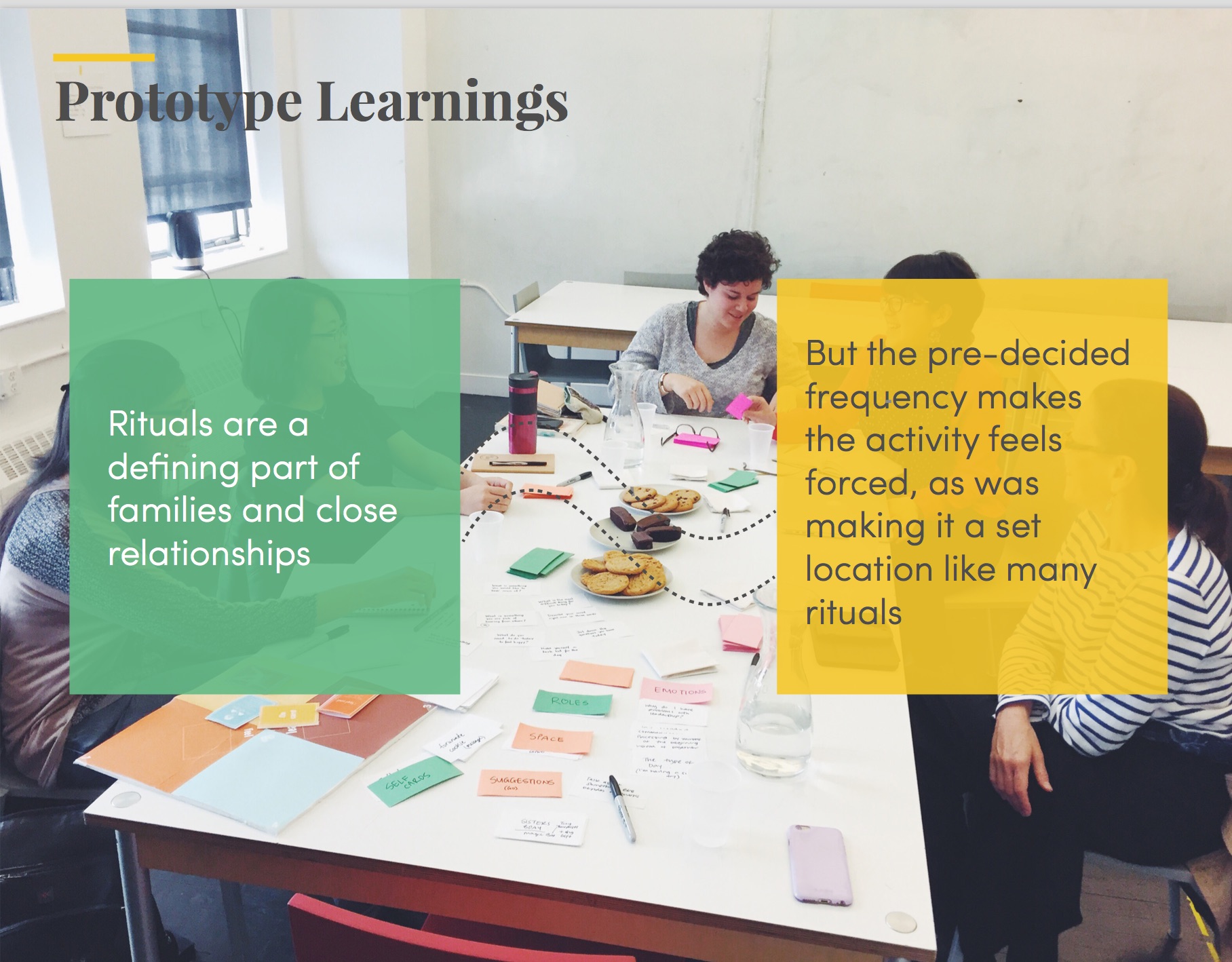
The cards were integrated at this point with a game board which corresponded to the cards, and a ritual of orders of cards was created. This felt a little too forced to have to go through a set number of cards every time the ritual took place, but the idea of an object as a way to help address stress in this situation was key.
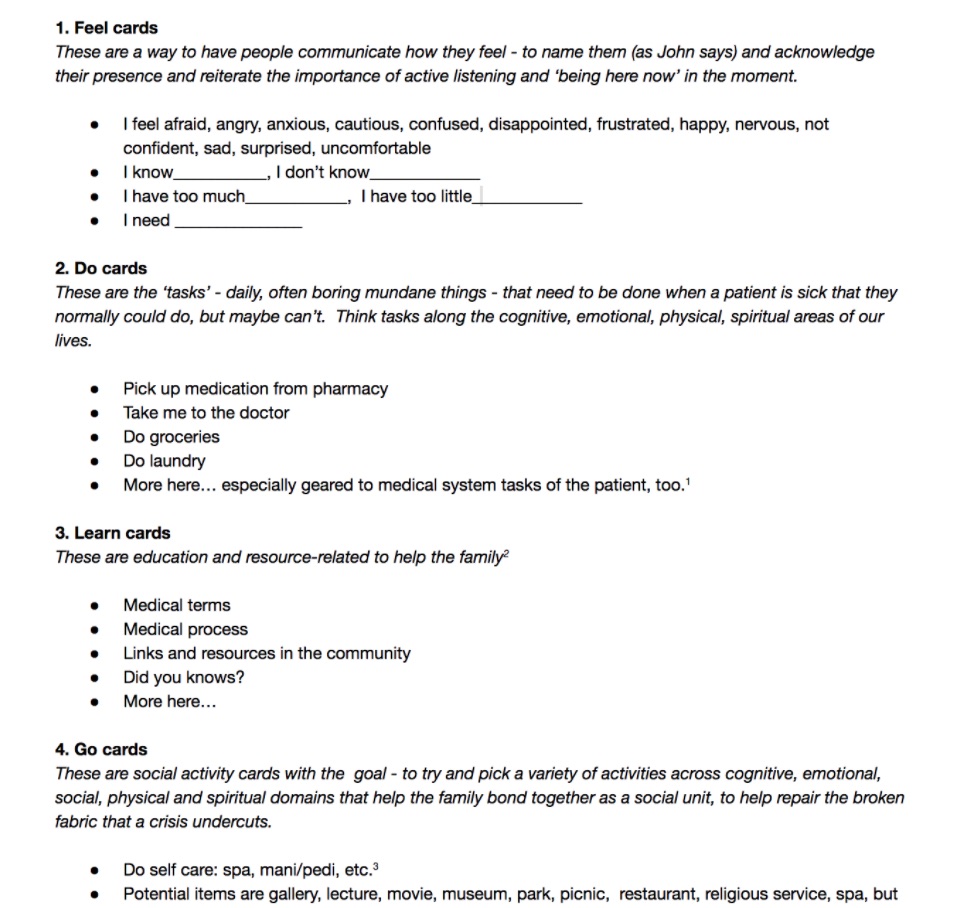
I created four categories of cards and started to create individual cards within each category that would correspond to a holistic view of the self, and people’s different emotional, intellectual, physical and spiritual needs.
We ran a workshop to test out our prototype and came up with takeaways that shaped our next prototype and ultimate design direction – including how to capture this in a ‘future state’ video demonstrating our proposed intervention. Image courtesy Ankita Roy.
Proposed intervention

Our design intervention is called Hum. Hum – which means ‘us’ in Hindi – is an experience designed to create moments between patients and their core circle of caregivers through engaging in meaningful activities together – a new kind of ritual for families. Rituals can encourage the fluidity of roles to cultivate shared leadership and family bonding and provide emotional support to both patients and their circle of caregiving, and a space for a life outside of illness to occur. (Branding courtesy Javiera Arenas, production of the Hum pack courtesy Ankita Roy).
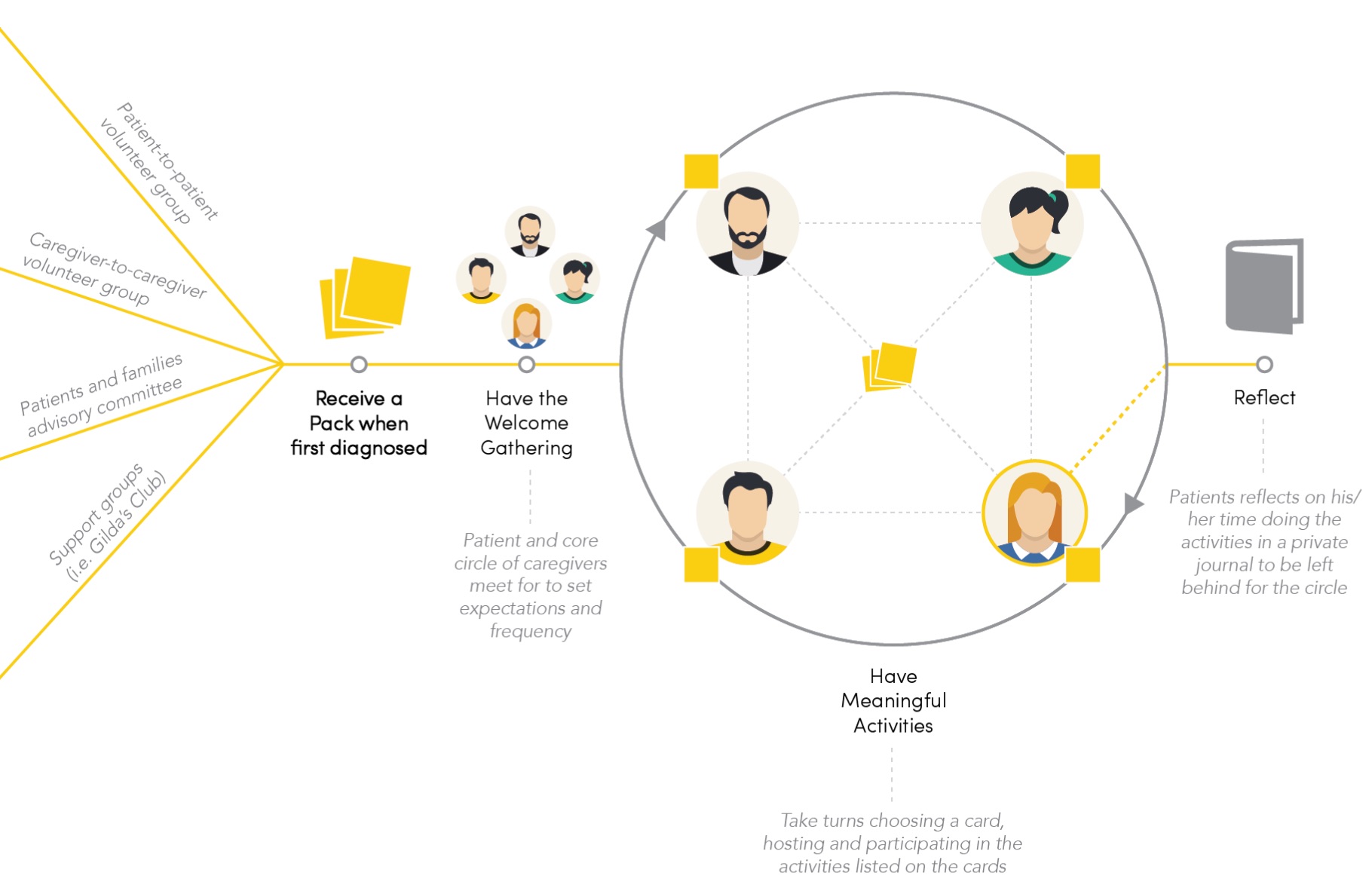
The Hum system
- The starting point: A patient receives a pack when first diagnosed – this can occur through multiple channels that we discovered through research. Caregivers and patients who have been through this experience are motivated to ‘give back’ by volunteering in our system
- Welcome gathering: Here we introduce Hum and start to integrate it into a care circle
- Activity cards: There are multiple categories of cards incorporated both present and future thinking activities, as well as past-centric activities (‘legacy’). The activities rotate – after each activity the person in charge of that week’s activity will give the card deck to someone else in the core circle, who will lead the next activity
- Journal for reflection: For the patient, after each activity documentation and personal reflection in a journal helps make meaning from the experience
Categories for the Hum cards
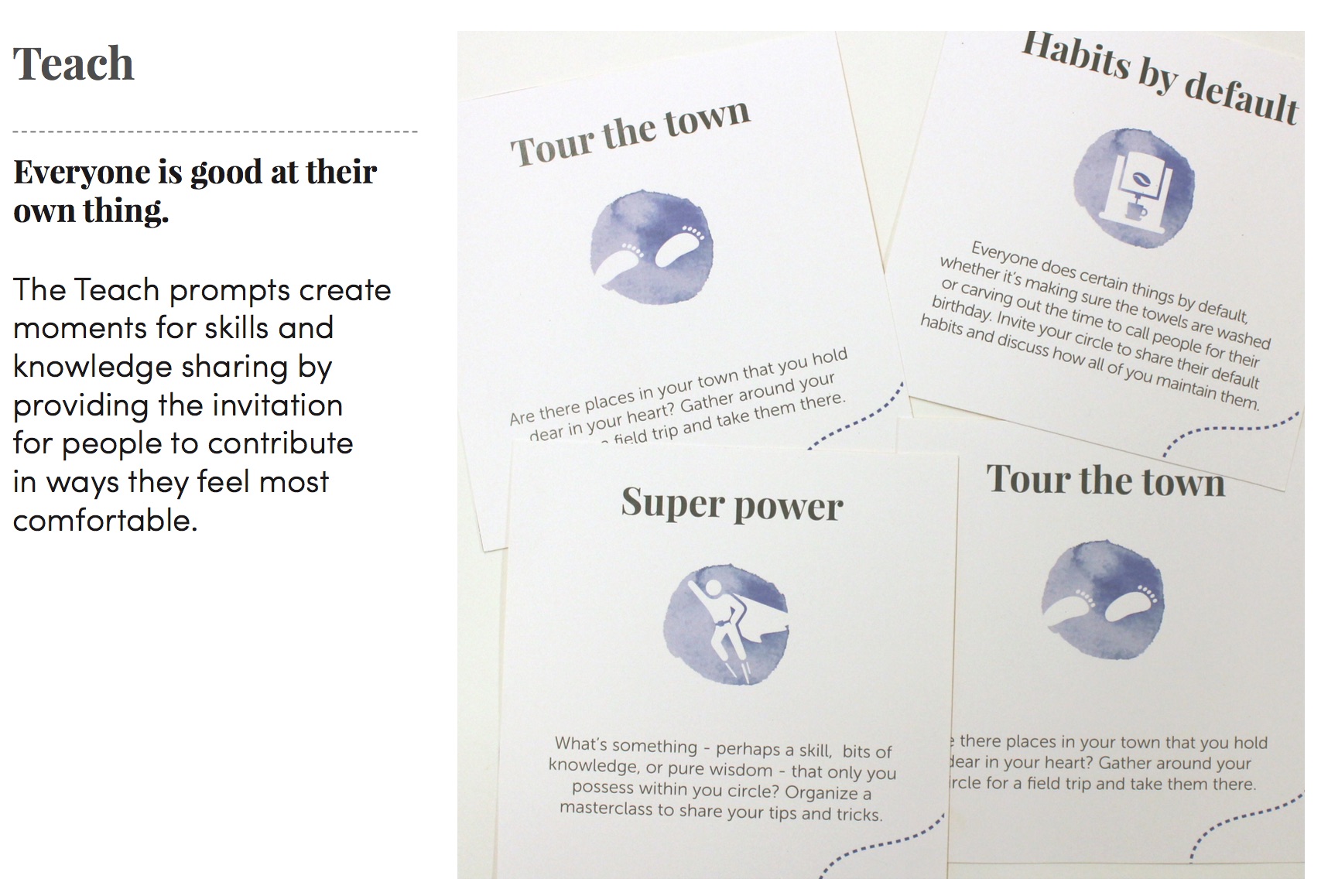
- Teach: In our research, we learned that patients who are the leading members of a family or social group can worry about what happens to the group once they are gone. Parents especially worry about knowledge transfer. The Teach Cards are geared to calm that worry by creating prompts to share skills and knowledge that go from being implicit for one person to shared wisdom amongst the group.
- Experience: This corresponds to new normals. Making time to do other everyday activities that bring people joy. Unfortunately, not everyone remembers to do that during illness. These prompts therefore serve as a reminder to continue to live one’s life.
- Legacy: We heard a story in one of the interviews that the patient wanted to take photos of all the nurses and doctors treating him before his move to hospice. Capturing memories together with leaving a legacy helps patients and caregivers create pauses to do that.
Teach: In our research, we learned that patients who are the leading members of a family or social group can worry about what happens to the group once they are gone. Parents especially worry about knowledge transfer. The Teach Cards are geared to calm that worry by creating prompts to share skills and knowledge that go from being implicit for one person to shared wisdom amongst the group.
This was the final set of categories for cards we presented, but we see a key part of this system as the expansiveness – so having user generated content to make this a living system that reflects its users. Cards for categories that respond to cultural sensitivities, different types of caregiver situations or different types of illnesses could occur to meet the needs of users
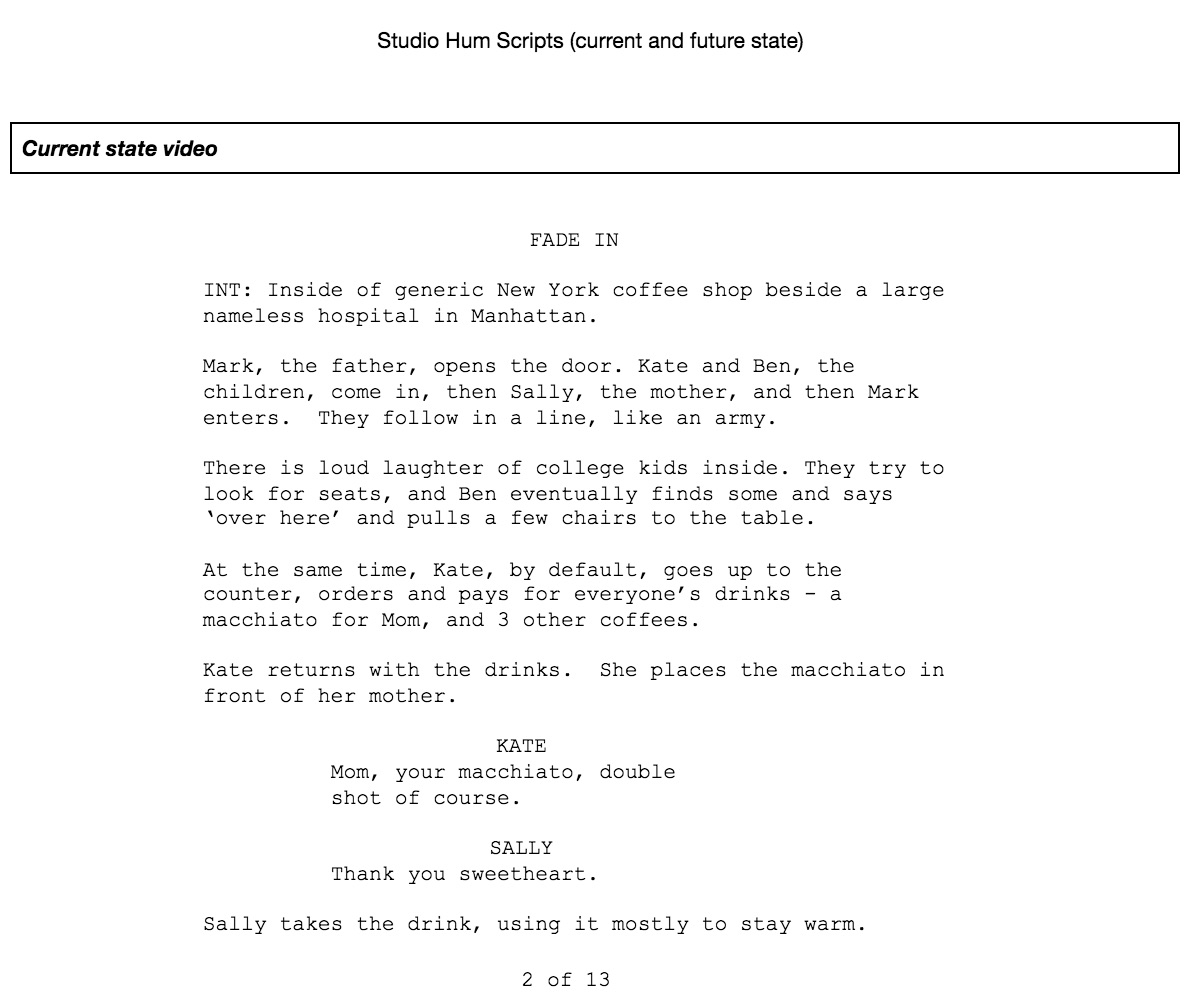
Telling the story of the Hum system through film
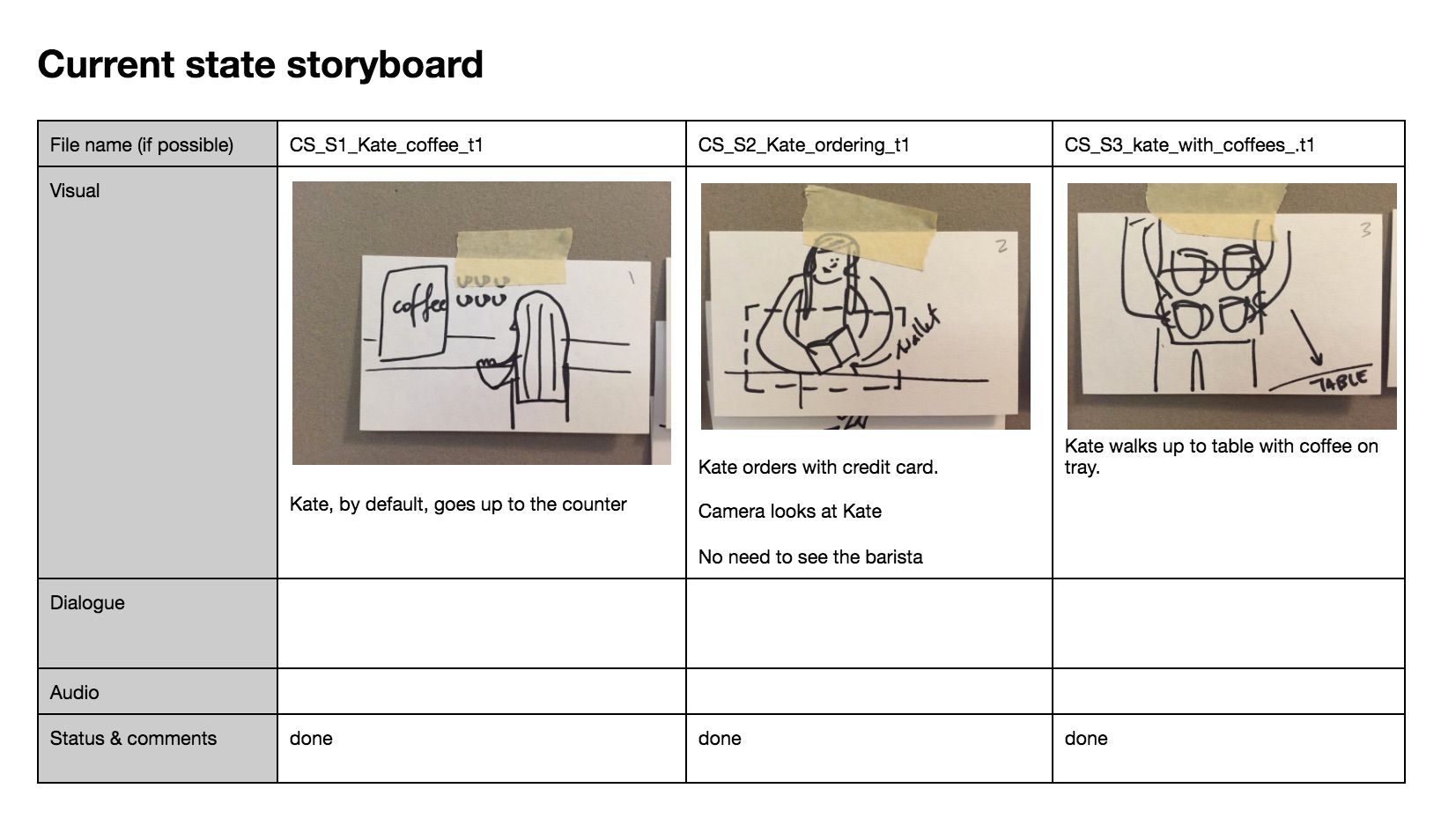
We also used film as an ethnographic method to understand the story of one such family dealing with a crisis. One of our incredible professors, John Bruce, was not only a strategist but a filmmaker and end of life doula. (Our other professor, Patty Beirne, was no less incredible – a visionary working in innovation at Memorial Sloan Kettering Cancer Care). The use of film for us as a team allowed us to tell a very personal story of one family’s struggle, the family unit being the focus of who Hum was there to assist. The concept was to show how an intervention would work in ‘the field’ rather than simply design a solution and assume our work is done. By embedding our work in a family unit such as this, and explore the issues on a more intimate scale using film we might begin to humanize our interventions. The use of film involved showing a ‘current state’ of a family in crisis, and an ‘ideal state’ after our design intervention. My role was to determine what kind of story we would write, write the script with my team, advise on the storyboard (which was documented by Javi), choose actors, direct the actors on the roles (walking them through emotional range required) produce the film (manage the project of day of shooting) ultimately editing the two films, selecting music and presenting it with the team for our final presentation.

I found myself casting a movie, and editing a movie and wondering how I got myself into this. (Kudos to Ankita who filled in the last minute when one of our actors dropped out).
It was an intense experience, and because our class wasn’t on filmmaking we could choose the fidelity and duration – we could use stop motion animation or any method we felt was best, and lots of footage of course was left on the cutting room floor. The concept of using film is something that excites me, especially for understanding interpersonal dynamics in a richer way.
Results
Hum offers promise on a number of levels, centered on the value of the activity cards and journal as much as the system itself:
- The Experience prompts: a reminder for patients and caregivers to continue doing things that bring them joy and to embrace the present.
- The Teach prompts: moments for skills and knowledge sharing by providing the invitation for people to contribute in ways they feel most comfortable.
- The Legacy prompts: a pause for storytelling, recounting memories and capturing the important moments in life.
- The Journal: creates an intentional space for the patient to reflect on the activities being done with the core circle.
Crisis and ruptures are also openings and opportunities. The end of life is not a problem to solve but rather an opportunity for patients, families and caregivers to make meaning in the face of mortality and find ways to live despite the situation.
The project was nominated by the studio’s professors and the Transdisciplinary Design department and is featured on the Parsons Web site as an example of ‘exemplary work’ and was featured as a case study in our professor, John Bruce’s book, Participatory Design and Social TransformationImages and Narratives of Crisis and Change.